Why Endometriosis Is Not 'Just a Bad Period': The Molecular Reality
1. Why the classic definition is misleading
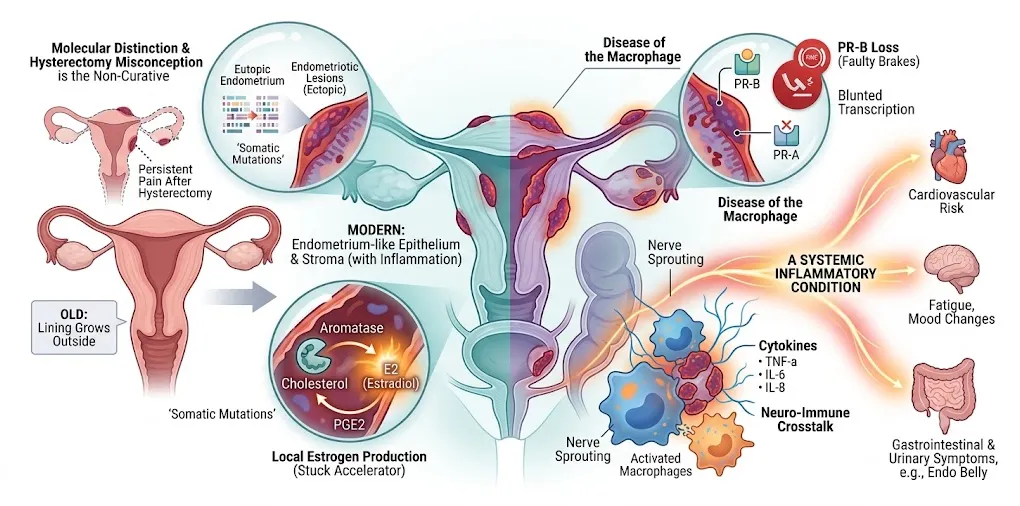
For decades, endometriosis was often described as “the lining of the uterus growing outside the uterus.” Modern consensus definitions instead describe it as a disease characterized by endometrium-like epithelium and/or stroma located outside the endometrium and myometrium, usually with an associated inflammatory process. This wording reflects the fact that lesion tissue only resembles, but is not identical to, normal uterine endometrium.
This seemingly small shift matters clinically. If the disease is framed as a simple displacement of uterine lining, it reinforces the idea that removing the uterus (hysterectomy) should be curative. In reality, persistent or recurrent pain and reoperation after hysterectomy—especially when ovaries or extra‑uterine lesions remain—are well documented, showing that endometriosis is not merely a uterine disease.
2. Endometrium‑like, but genetically and phenotypically distinct
Histologically, endometriotic lesions contain glands and stroma that resemble endometrium, which explains the historical terminology. At the molecular level, however, lesion epithelium frequently harbors somatic mutations and shows clonal expansion patterns distinct from matched eutopic endometrium, supporting the idea that lesions are related to but biologically distinct from the uterine lining.
Eutopic endometrium from women with endometriosis also differs from that of unaffected women, including altered ultrastructure, glycosylation patterns, and gene expression linked to adhesion, invasion, and immune modulation. Together, these findings challenge simplistic definitions and justify describing lesions as “endometrium‑like” rather than true endometrium.
3. Local estrogen production and intracrine signaling
Endometriosis is estrogen dependent, but lesion biology cannot be fully explained by circulating hormone levels alone. Stromal cells in endometriotic tissue express aromatase (CYP19A1) and other steroidogenic enzymes required for de novo estradiol synthesis from cholesterol, which are largely absent in normal endometrium. Prostaglandin E₂ signaling upregulates aromatase, creating a local positive feedback loop that maintains high intralesional estrogen.
This intracrine estrogen production means that lesions can sustain estrogen‑driven growth and inflammation even when serum estrogen appears “normal,” providing a mechanistic rationale for therapies targeting local steroid metabolism (for example, aromatase inhibitors or drugs aimed at intracrine pathways).
4. Progesterone resistance: the “broken brakes”
Progesterone normally counterbalances estrogen by limiting proliferation, promoting differentiation, and exerting anti‑inflammatory effects in the endometrium. In endometriosis, multiple studies demonstrate reduced expression of progesterone receptor (PR)—particularly the PR‑B isoform—and an altered PR‑A/PR‑B ratio in both eutopic and ectopic tissues. Promoter hypermethylation of the PR‑B gene has been identified as one mechanism underlying this loss.
Functionally, this translates into blunted transcriptional responses to progesterone and partial resistance to progestin therapy in some patients. Describing the system as a “stuck accelerator” (local estrogen) with “faulty brakes” (progesterone resistance) is therefore a reasonable metaphor for this endocrine imbalance.
5. Macrophages, cytokines, and neuro‑immune pain
The peritoneal environment in endometriosis is characterized by increased numbers of activated macrophages and elevated concentrations of inflammatory mediators such as TNF‑α, IL‑6, IL‑8, VEGF and others. Rather than clearing ectopic tissue, these macrophages support lesion survival, angiogenesis, and innervation, leading some authors to describe endometriosis as a “disease of the macrophage.”
Inflammatory cytokines and growth factors sensitize peripheral nociceptors and promote sprouting of nerve fibers within and around lesions. This neuro‑immune crosstalk helps explain why endometriosis pain can be severe, chronic, and disproportionate to lesion size, and why symptoms often include deep dyspareunia, dyschezia, and pain beyond menstruation.
6. A systemic inflammatory disease, not just “bad periods” or GI trouble
Beyond pelvic pain and heavy menstruation, endometriosis is increasingly recognized as a chronic systemic inflammatory condition. People with the disease show evidence of systemic immune activation, oxidative stress, and altered inflammatory biomarkers, and they appear to carry elevated risks of several comorbidities, including cardiovascular and metabolic disorders. Fatigue, mood changes, and widespread pain are commonly reported clinical features.
Gastrointestinal and urinary symptoms—such as bloating (often described as “endo belly”), constipation, diarrhea, dyschezia and dysuria—are frequent, especially in deep infiltrating or bowel/urinary tract disease, but they represent only one facet of a broader, multi‑system disorder. Conceptualizing endometriosis purely as a “bad period” or a localized gynecological or gastrointestinal problem therefore underestimates its systemic, immune‑driven nature.
References
- Tomassetti C, Johnson NP, Petrozza JC, et al. An international terminology for endometriosis, 2021. Hum Reprod Open. 2021;2021(4):hoab029. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC8530702/
- Namnoum AB, Hickman TN, Goodman SB, Gehlbach DL, Rock JA. Incidence of symptom recurrence after hysterectomy for endometriosis. Fertil Steril. 1995;64(5):898–902. Available at: https://pubmed.ncbi.nlm.nih.gov/7589631/
- Zondervan KT, Becker CM, Missmer SA. A lifelong impact of endometriosis: pathophysiology and clinical implications. Nat Rev Endocrinol. 2023;19(4):213–228. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC10139092/
- Suda K, Nakaoka H, Yoshihara K, et al. Clonal expansion and diversification of cancer‑associated mutations in endometriosis and normal endometrium. Cell Rep. 2018;24(7):1777–1789. Available at: https://linkinghub.elsevier.com/retrieve/pii/S2211124718311276
- Noë M, Ayhan A, Wang T‑L, Shih I‑M. Distinct developmental trajectories of endometriotic epithelium and stroma: implications for the origins of endometriosis. J Pathol. 2018;246(3):329–340. Available at: https://pubmed.ncbi.nlm.nih.gov/30015393/
- Jones CJP, Nardo LG, Litta P, Fazleabas AT, Luck MR. Eutopic endometrium from women with endometriosis shows altered ultrastructure and glycosylation compared with controls. Reprod Sci. 2009;16(6):559–568. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC5098404/
- Khan KN, Kitajima M, Hiraki K, et al. The eutopic endometrium in endometriosis. Fertil Steril. 2012;98(3):511–519. Available at: https://pubmed.ncbi.nlm.nih.gov/22417665/
- Bulun SE, Zeitoun K, Takayama K, Noble L. Aromatase and other steroidogenic genes in endometriosis. Hum Reprod Update. 2000;6(2):108–123. Available at: https://academic.oup.com/humupd/article/12/1/49/607182
- Rocha A, Reis FM, Petraglia F. Is intracrinology of endometriosis relevant in clinical practice? A systematic review on estrogen metabolism. Front Endocrinol (Lausanne). 2022;13:950866. Available at: https://www.frontiersin.org/articles/10.3389/fendo.2022.950866/full
- Wu Y, Halverson G, Basir Z, Strawn E, Yan P, Guo S‑W. Promoter hypermethylation of progesterone receptor isoform B (PR‑B) in endometriosis. Epigenetics. 2006;1(2):106–111. Available at: https://pubmed.ncbi.nlm.nih.gov/17965625/
- Patel BG, Lenk EE, Lebovic DI, Shu Y, Yu J, Taylor RN. Progesterone resistance in endometriosis: estrogen receptor‑beta and inflammation. Semin Reprod Med. 2010;28(1):36–43. Available at: https://pubmed.ncbi.nlm.nih.gov/20104427/
- Harada T, Iwabe T, Terakawa N. Role of cytokines in progression of endometriosis. Gynecol Obstet Invest. 1999;47 Suppl 1:34–39. Available at: https://pubmed.ncbi.nlm.nih.gov/10087426/
- Bedaiwy MA, Falcone T. Peritoneal fluid environment in endometriosis. Obstet Gynecol Clin North Am. 2003;30(1):69–82. Available at: https://pubmed.ncbi.nlm.nih.gov/12854733/
- Berbic M, Fraser IS. Endometriosis, a disease of the macrophage. Front Biosci (Elite Ed). 2013;5:577–586. Available at: https://www.frontiersin.org/articles/10.3389/fimmu.2013.00009/full
- Rocha ALL, Reis FM, Taylor HS, et al. Endometriosis as a model of systemic inflammation: clinical, molecular and translational implications. Int J Endo Metab Disord. 2025; (in press). Available at: https://ieccmexicojournal.com/index.php/publishing/article/view/35
- Hvidtfeldt D, et al. Endometriosis and long‑term cardiovascular risk: a nationwide Danish study. Eur Heart J. 2024;45(44):4734–4746. Available at: https://academic.oup.com/eurheartj/article/45/44/4734/7741666
- World Health Organization. Endometriosis: fact sheet. WHO; 2025. Available at: https://www.who.org/news-room/fact-sheets/detail/endometriosis